Article Text

Abstract
Objective To investigate the roles of mobile health, or mHealth, in the psychosocial health of pregnant women and mothers.
Methods A systematic search was conducted in databases and grey literature including MEDLINE, Web of Science, CINAHL, PsycINFO, PsycARTICLES, Academic Search Complete, SocINDEX, Central Register of Controlled Trials, The Database of Abstracts of Reviews of Effects, NHS Economic Evaluation Database, Health Technology Assessment, UNICEF and WHO databases. Two searches were conducted to include original research articles published in English until 15 November 2021. Several tools were used to assess the risk of bias: revised Cochrane risk of bias tool for randomised trials, Risk of Bias in Non-randomized Studies of Interventions, National Heart, Lung, and Blood Institute quality assessment tool for cohort and cross-sectional studies, Critical Appraisal Skills Program checklist for qualitative studies and Mixed Methods Appraisal Tool for mixed-methods studies. Certainty of evidence was assessed using Grading of Recommendations Assessment, Development and Evaluation approach. Due to the high heterogeneity and variability of the included studies, data synthesis was conducted narratively.
Results 44 studies were included among 11 999 identified articles. Most studies reported mixed findings on the roles of mHealth interventions in the psychosocial health of pregnant women and mothers; mHealth improved self-management, acceptance of pregnancy/motherhood and social support, while mixed results were observed for anxiety and depressive symptoms, perceived stress, mental well-being, coping and self-efficacy. Furthermore, pregnant women and mothers from vulnerable populations benefited from the use of mHealth to improve their psychosocial health.
Conclusions The findings suggest that mHealth has the potential to improve self-management, acceptance of pregnancy/motherhood and social support. mHealth can also be a useful tool to reach vulnerable pregnant women and mothers with barriers to health information and facilitate access to healthcare services. However, the high heterogeneity limited the certainty of evidence of these findings. Therefore, future studies should identify the context under which mHealth could be more effective.
- public health
- maternal medicine
- education & training (see medical education & training)
- international health services
- adult psychiatry
- mental health
Data availability statement
All data relevant to the study are included in the article or uploaded as supplemental information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- public health
- maternal medicine
- education & training (see medical education & training)
- international health services
- adult psychiatry
- mental health
Strengths and limitations of this study
The current study comprehensively reviewed evidence on the roles of mobile health in the psychosocial health of pregnant women and mothers by including multiple domains of psychosocial health outcomes.
The study followed Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols guidelines and Synthesis Without Meta-analysis guidelines.
The high heterogeneity and uncertainty across the studies regarding the setting, study design and outcome measures make it difficult to draw firm conclusions.
Only English databases and articles were included in the review and may have limited the interpretation of the study findings.
Introduction
Psychosocial health refers to the inter-relations of the social environment and psychological health of an individual.1 2 It is multidimensional and covers areas such as depression, stress, self-sufficiency and social support.3 During the pregnancy and postpartum period, women are especially vulnerable to facing psychological problems, particularly stress and anxiety disorder with comorbidity of depression.4–6 According to a study that systematically reviewed the global prevalence of antenatal and postnatal anxiety, 19.4% of pregnant women experienced antenatal anxiety across the three trimesters and 13.7% of mothers experienced postnatal anxiety in the first 6 months following delivery in high-income countries.7 In low-income and middle-income countries, the prevalence was significantly higher—34.4% and 25.9%, respectively.7 Experiencing pregnancy and childbirth, especially for the first time, is a drastic transition for women as they grow into the role of becoming a mother.8 This psychological ambivalence can cause problems for both pregnant women and mothers. Furthermore, psychosocial health among pregnant women is crucial for their well-being and the health of the infant. Anxiety during pregnancy has been associated with adverse effects on infants’ and children’s development, including premature birth, hyperactivity, cleft lip and impaired brain development.9 10
Using mobile health (mHealth) to deliver pregnancy and postpartum care health services has become more familiar with the advancement of information and communication technologies. mHealth can be delivered through various electronic devices, such as mobile phones, tablet computers, personal digital assistants, and other wearable devices or wireless infrastructure. It is an effective tool to deliver perinatal care interventions because of its cost-effectiveness and scalability, which can benefit both the individual users and the health system.11 12 Moreover, delivering interventions via mobile devices is beneficial because of their computational power, portability and price, and the tendency of owners to keep them nearby at all times.13 Due to these advancements and the increasing use of mobile phones and the internet, pregnant women and mothers rely on the internet and mHealth applications (apps) to seek sources of health information and services for self-care and child care for a multitude of reasons, such as their desire to connect with other women going through the same experiences and instant professional consultation and reassurance at little or no cost.14 mHealth apps can also support pregnant women and mothers to manage their own health, promote a healthy lifestyle, and encourage access to information at any time and place.15
Despite the potentials of mHealth, there are also its challenges that remain to be tackled. In low-resource settings, potential barriers to mHealth interventions include the limited level of literacy, access to mobile data, knowledge of technology, cultural beliefs and availability of mobile devices.16 The culture and cultural beliefs surrounding the women may have restricted opportunities to learn about technology and therefore limited their skills to navigate mobile services. Other barriers include unstable power supply and poor infrastructure and connectivity to internet, especially in rural or conflict-affected areas.17 18 Furthermore, due to the variability in the quality of mHealth services, pregnant women’s and mothers’ distrust and worry on the security issues and lack of evidence-based information provided to them could also act as a barrier in mHealth interventions.19
A study by Dol et al systematically reviewed the impact of mHealth interventions during the perinatal period on maternal psychosocial health outcomes.20 The findings suggest that mHealth interventions for supporting breastfeeding and newborn care practices that could improve perceived social support and interventions targeting postpartum depression had an impact in reducing postpartum depression. However, the review included only four psychosocial health outcomes: self-efficacy, social support, anxiety and depression. Although they are considered as common psychosocial health outcomes, other aspects of psychosocial health, such as perceived stress and coping that are often experienced during the perinatal period, should also be considered. Moreover, the review included studies with either a quasi-experimental or randomised controlled study design and focused exclusively on high-income countries. They may have missed valuable information on the advantages and disadvantages of mHealth interventions among pregnant women and mothers that could be observed only through observational and qualitative studies. In addition, it makes it challenging to comprehensively understand the global situation of mHealth interventions in the field of maternal and child health when excluding studies from low-income and middle-income countries.
Furthermore, several other systematic reviews and meta-analyses have also investigated the effectiveness of mHealth on pregnancy and postpartum care. The findings showed that using mHealth to support pregnancy and postpartum care was feasible and appropriate. However, the reviews focused on the roles of mHealth in clinical/health outcomes,14 21 lifestyle behaviours22 or the specific perinatal period.23 Some reviews were conducted only among either low/middle-income countries or high-income countries24–26 or a specific type of mHealth service, such as mobile apps or short messaging services (SMS).14 15 22 24 Therefore, this study aimed to review evidence from all studies designs conducted in countries of varying income levels to comprehensively investigate the roles of mHealth in the psychosocial health of pregnant women and mothers.
Methods
Patient and public involvement
Patients and/or the public were not involved in the current systematic review.
Search strategy
The current systematic review initially followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) reporting guidelines (see online supplemental file 1).27 It was written in accordance with the registered review protocol on PROSPERO (no. CRD42020188975) (see online supplemental file 2). Eleven online bibliographical databases were searched: MEDLINE, Web of Science, CINAHL, PsycINFO, PsycARTICLES, Academic Search Complete, SocINDEX, Cochrane Central Register of Controlled Trials, The Database of Abstracts of Reviews of Effects, NHS Economic Evaluation Database and the Health Technology Assessment. Grey literature from the UNICEF and WHO databases was also searched. The first two authors (JLS and RRC) developed the search strategy in MEDLINE using a combination of Medical Subject Headings terms and keywords (see online supplemental file 3) and applied no date restriction. The search strategy was improved after using article identification numbers to maximise the sensitivity and specificity for identifying relevant articles. The search was conducted at two time points where the initial search was conducted on 31 May 2020 and an updated search on 15 November 2021. Included in the search were original research articles written in English published on or before 15 November 2021. The reference lists of eligible articles were manually searched to screen for additional studies.
Supplemental material
Supplemental material
Supplemental material
Eligibility criteria
The studies were considered eligible if they described or delivered an mHealth intervention (eg, through mobile apps or SMS) targeted to improve at least one aspect of psychosocial health (eg, depression, stress, anxiety, social support, self-efficacy) among pregnant women and mothers of infants and children aged 0–5 years. Exclusion criteria were mHealth interventions that (1) were not mobile or tablet based and (2) did not focus on psychosocial health outcomes. We did not include eHealth interventions, such as telemedicine and telehealth interventions that were not exclusively delivered via portable and handheld devices. For example, interventions using telephone for delivering interventions were excluded for the reason that telephones could indicate either cell phones or landline telephones, or both. Eligible study designs included randomised controlled trials (RCTs), quasi-experimental, cohort, observational, cross-sectional and other comparative studies, as well as case studies and evaluation reports. Letters, editorials, reviews, conference abstracts and posters, dissertations and books were excluded. All eligible studies found on the databases were exported to the reference-managing software EndNote to facilitate the study selection process and screen for duplicate records.
Data extraction
After removing the duplicates, the first two authors (JLS and RRC) screened the titles and abstracts of identified studies for relevance. Next, full-text copies of papers were assessed for eligibility by three authors (JLS, RRC and MK), with any disagreements resolved through discussions; if a consensus was not reached, a fourth author was brought in for discussion at each stage (AS or MJ). Finally, the original three authors (JLS, RRC and MK) extracted data using a standardised extraction form following the Population, Intervention, Comparison and Outcome format on Microsoft Excel to ensure the capture of all necessary information, including title, citation (author, publication, year and source), study area, study objectives, study design, study setting, study population, sample size, types of mHealth interventions, comparison group and summary of reported outcomes.
Risk of bias assessment and certainty of evidence
After data extraction, three authors (JLS, RRC and MK) independently assessed the risk of bias and methodological rigour of the included studies. Revised Cochrane risk of bias tool for randomised trials (RoB 2.0) developed by Cochrane Collaboration for RCTs28 was used to assess RCT-designed studies. The RoB 2.0 tool comprises a series of signalling questions that elicited information on the features of RCTs relevant to assessing the risk of bias. Once the signalling questions were answered, the RCTs were judged and assigned as low, some concerns or high risk of bias. For non-RCTs, four of the following tools were used for the risk of bias assessment: Risk of Bias in Non-randomized Studies of Interventions for non-randomised studies of intervention,29 National Heart, Lung, and Blood Institute quality assessment tool for cohort and cross-sectional studies,30 Critical Appraisal Skills Program checklist for qualitative studies31 and Mixed Methods Appraisal Tool for mixed-methods studies.32 Any disagreements were settled through discussion to arrive at a consensus among the reviewers. The certainty of the evidence was assessed using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach.33
Data synthesis
Due to the broad inclusion criteria, high heterogeneity was observed among the included studies regarding the study designs, measurement tools, statistical analyses and outcomes. Therefore, the current review did not pursue a meta-analysis. Instead, we used Synthesis Without Meta-analysis reporting guidelines (see online supplemental file 4) to conduct data synthesis.34 A detailed examination was conducted on the numerical and textual summary findings of the included studies. Findings were then synthesised narratively and the studies were grouped according to psychosocial health outcomes. Summary of findings was presented in a table including psychosocial health outcomes, types of mHealth services, total number the outcome was reported, and whether the finding had no effect, mixed effect, or positive effect. Conclusions were reached in each study for the effects of mHealth intervention. We considered an outcome to have a ‘positive effect’ if the mHealth intervention showed a significant effect (eg, improvement in anxiety/depressive symptoms, increase in mental well-being/self-efficacy) and narrative findings indicated positive results (ie, benefits of using mHealth services). An outcome was considered to have a ‘mixed effect’ when it showed positive changes but were not necessarily statistically significant (eg, Multidimensional Scale of Perceived Social Support mean score: pre-intervention 23.3, post-intervention 25.0, p=0.80). When there was no significant effect and narrative findings reported negative results, the outcome was considered as ‘no effect’.
Supplemental material
Results
Study selection
A total of 11 999 records were identified from all the databases, grey literature and through hand-search at two time points. After removing the duplicates, 11 120 records were retained. Of these, 135 articles were identified as potential studies for inclusion. The reviewers then assessed the full text of the identified studies and excluded 91 articles (see online supplemental file 5). Finally, a total of 44 articles were included in the final data synthesis. The screening process is depicted in the PRISMA flow diagram (figure 1).
Supplemental material

Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow chart.
Risk of bias and methodological rigour of included studies
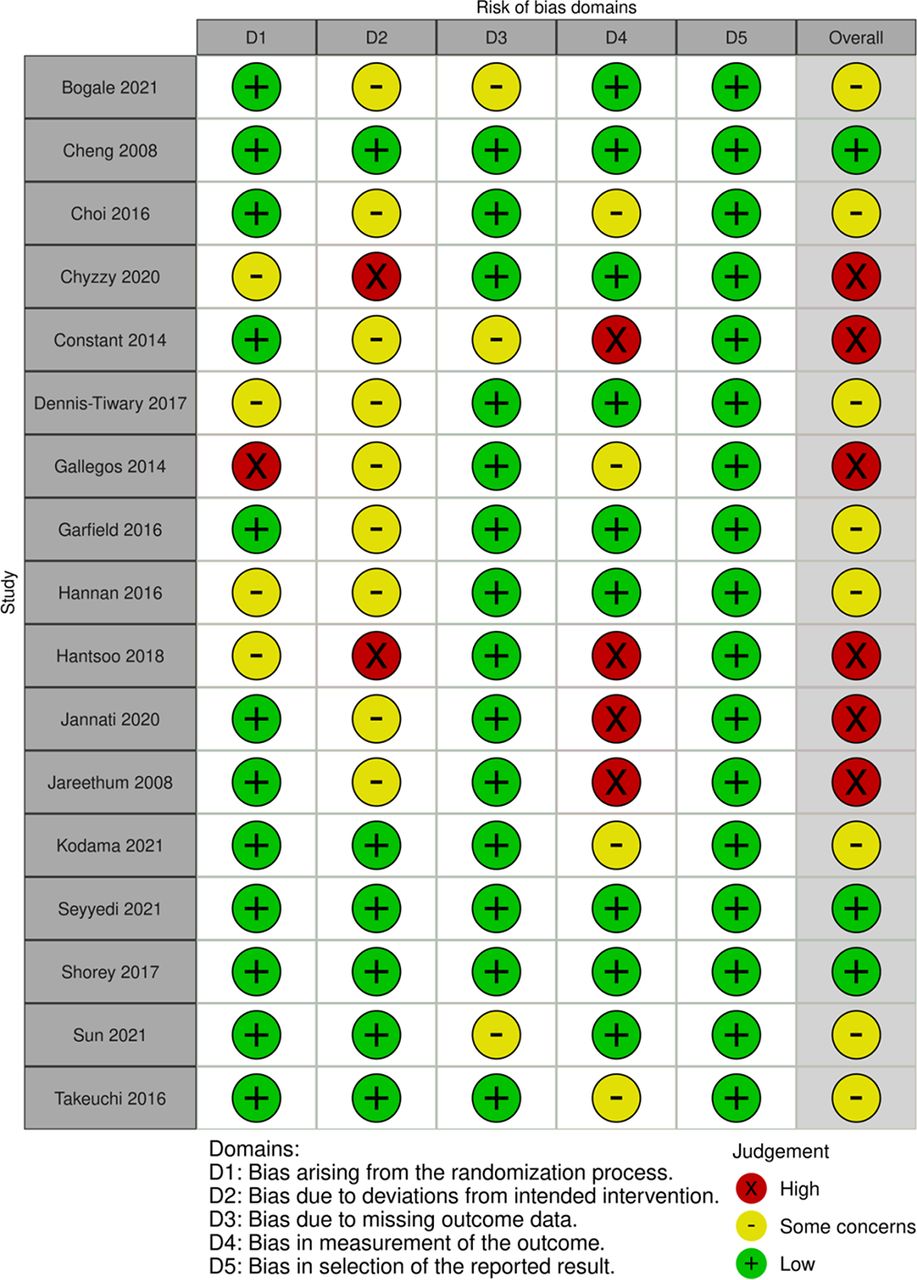
The risk of bias and the methodological rigour varied across the included studies. Forty-four studies were eligible for the assessment of methodological quality. Out of 44 studies, 17 studies were RCTs35–51 and their risk of bias assessment is depicted in figure 2.52 Six out of 17 RCTs were assessed as having a high overall risk of bias due to bias arising from randomisation process, deviations from the intended intervention and unclear measurement outcome.38 39 41 44–46 Most of the studies were assessed as having some concerns for mainly not being able to blind the participants/outcome assessors due to the nature of the intervention conducted in the studies.35 37 40 42 43 47 50 51 The remaining three studies were considered low risk of bias.36 48 49

{kind=link}
{kind=link}
Risk of bias summary for randomised controlled trials based on authors’ judgements (low, some concerns, high) about each risk of bias item of the included study.
Online supplemental file 6 shows the results of the risk of bias assessment for the non-RCTs. Among the 11 quasi-experimental studies, 4 had a serious risk of bias,53–56 4 had a moderate risk57–60 and 3 were assessed as low risk.61–63 The two observational studies did not have clear information on confounding variables and blinding of the outcome assessors.64 65 A few studies among the seven qualitative studies66–72 lacked information on the positionality of researchers and potential bias may have risen due to the recruitment strategy. Seven mixed-methods study73–79 also did not provide any information on confounding. Furthermore, online supplemental file 7 shows the results of the GRADE certainty of evidence assessment.
Supplemental material
Supplemental material
Study characteristics
The summary of study characteristics is presented in online supplemental file 8.
Supplemental material
Study countries
The World Bank income level classification as of June 2021 was incorporated to categorise the countries according to their income level.80 Most of the included studies were conducted in high-income countries (31 of 44; 70%), including the US (n=15), Australia (n=3), Japan (n=3), UK (n=2), Singapore (n=1), Taiwan (n=1), Israel (n=1), Norway (n=1), Korea (n=1), Italy (n=1), Canada (n=1) and Germany (n=1). Six studies (6 of 44; 14%) were conducted in upper middle-income countries: South Africa (n=1), Turkey (n=1), Thailand (n=1), China (n=1), Brazil (n=1) and Dominican Republic (n=1). Six studies (6 of 44; 14%) were conducted in lower middle-income countries: Iran (n=2), Kenya (n=1), Zambia (n=1), India (n=1) and Palestine (n=1). Only one study (1 of 44; 2%) was conducted in a low-income country, Uganda (n=1).
Study participants
A slight majority of the studies recruited pregnant women (26 of 44; 59%) and the recruited population varied from generally healthy pregnant women to at-risk pregnant women. Other studies recruited mothers (14 of 44; 32%), including adolescent mothers and mothers who screened positive for perinatal depression. Few studies recruited both pregnant women and mothers (4 of 44; 9%). The inclusion criteria for the gestational age of pregnant women and the timeline of the perinatal period varied across studies.
Types of mHealth services and interventions
There were differences in the mHealth technologies used to facilitate interventions. Twenty-six studies used mobile apps (26 of 44; 59%) while 11 used SMS (11 of 44; 25%). Two studies used both SMS and voice calling on mobile phones (2 of 44; 5%). A few of the mHealth interventions were delivered using other mHealth services, such as instant messaging services (eg, WhatsApp Messenger) (2 of 44; 5%), e-learning service via cellphone internet (1 of 44; 2%), smartphone website (1 of 44; 2%) and mobile-based interactive voice response system (1 of 44; 2%).
The types of mHealth interventions were widely diverse. The interventions were categorised into 10 types incorporating the mHealth and Information and Communications Technology (ICT) Framework81 and its adaptation.21 Studies were counted in more than one category type if the mHealth intervention included multiple functions. The 10 types include health education or promotion (19 of 44; 43%), communication and support (15 of 44; 34%), psychoeducation or therapy (11 of 44; 25%), self-monitoring system (6 of 44; 14%), reminders (4 of 44; 9%), decision guideline (3 of 44; 7%), behaviour change (3 of 44; 7%), laboratory results (1 of 44; 2%), registries/vital events tracking (1 of 44; 2%) and electronic health records (1 of 44; 2%).
Study outcomes
In total, 77 comparisons were made across the 44 included studies that examined the roles of mHealth interventions in psychosocial health outcomes among pregnant women and mothers (see table 1). Some studies assessed multiple psychosocial health outcomes. Therefore, results are reported based on the number of comparisons made for each outcome.
Summary of the effect of mHealth interventions on psychosocial health outcomes of pregnant women and mothers
Anxiety symptoms
Thirteen studies assessed the roles of mHealth in anxiety symptoms among pregnant women and mothers.35 36 39 40 44 46 47 50 54 61–63 73 Four studies found positive effects, six studies had mixed findings and three studies found no significant effect (GRADE certainty of evidence: low). Jareethum et al conducted an RCT study in Thailand which sent two SMS messages per week containing information and warnings on abnormal symptoms appropriate to the women’s gestational age.46 As a result, pregnant women who received an SMS had lower anxiety levels during the antenatal and perinatal period than those who did not receive any SMS; however, it was only significant during the antenatal period (M=2.78 vs 4.93, p=0.002). Another RCT study conducted by Constant et al in South Africa sent 13 automated text messages with reminders to take medication and information about side effects to women undergoing medical abortion.40 Between baseline and follow-up, women who received the messages reported a decrease in their Hospital Anxiety and Depression Scale (HADS) score compared to the control group (M=11.40 vs 7.80, p=0.013).39
A pilot RCT conducted by Dennis-Tiwary et al in the US investigated the effectiveness of an attention bias modification training app to reduce pregnancy threat, anxiety and stress, and did not find any significant changes in the anxiety domain of Depression, Anxiety and Stress Scale between intervention (M=3.20, SD=3.00) and control group (M=2.07, SD=3.60) at 1-month follow-up.40 They also did not find any change in the Hamilton Anxiety Scale scores between intervention (M=9.20, SD=6.71) and control groups (M=6.93, SD=9.10). Similarly, Baumel et al conducted a quasi-experimental study to examine the effectiveness of an app that provided self-help tools and emotional support delivered by trained volunteers to pregnant women diagnosed with postpartum depression. They found no significant changes in the Beck Anxiety Inventory (BAI) scores between baseline (M=20.47, SD=13.15) and at 1-month follow-up (M=16.65, SD=7.52, p=0.11).61
Depressive symptoms
Twelve studies assessed the roles of mHealth in self-reported levels of depressive symptoms.37 44 45 49 50 54–56 60 61 63 70 Five studies found a positive effect, four studies had mixed findings and three studies found no significant effect (GRADE certainty of evidence: low). Song et al conducted a quasi-experimental study to test the effectiveness of a two-way text-messaging system to distribute health-related information to pregnant women with low socioeconomic status living in the US. They reported a reduction in the Center for Epidemiological Studies Scale score after the intervention (t (19)=2.991, p<0.01).55
Mixed results were reported among studies assessing the roles of mHealth in improving depressive symptoms using the Edinburgh Postnatal Depression Scale (EPDS). In Singapore, Shorey et al examined the effectiveness of a psychoeducational app to improve parenting outcomes. Parents in the intervention group reported no significant difference in the EPDS scores compared with the control group (Mean difference =7.00 vs 7.60).49 Similarly, Dalton et al reported no changes in EPDS scores between intervention and control group (detailed results of analyses not reported) and when comparing pre-intervention and post-intervention (M=6.08 vs 5.66, p=0.635).54 However, Baumel et al reported significant decline in EPDS scores after conducting an intent-to-treat analysis from baseline (M=17.32, SD=5.96) and after 30-day follow-up (M=13.53, SD=4.65, p=0.005). Beck Depression Inventory II scores also significantly improved (M=26.11, SD=13.34; M=19.18, SD=9.23, p=0.01).61
Perceived stress
Perceived stress was assessed in seven studies.39 40 43 50 55 59 60 Three studies found positive effects, two studies had mixed findings and two studies found no significant effect (GRADE certainty of evidence: very low). Constant et al reported lower scores on the Impact of Event Scale-Revised, which indicated lower levels of emotional stress (β=−1.8, 95% CI=−3.2 to −0.4, p=0.015) among the intervention group than those in the control group when adjusted for baseline anxiety.39 Furthermore, Jallo et al conducted a quasi-experimental study to investigate the effectiveness of a stress coping app to reduce stress in a sample of pregnant women staying in an obstetrical antepartum high-risk unit. They reported an immediate drop in their Visual Analog Stress Scale score when comparing before and after listening to the app with guided imagery audio (M=44.13 vs 22.04, p<0.0001). However, no differences were found when comparing Perceived Stress Scale scores between pre-intervention and post-intervention (median score=22.0 vs 22.0, p=0.750).59
Mental well-being
Two studies assessed mental well-being.55 64 One study found a positive effect, while one study did not find any significant effect (GRADE certainty of evidence: very low). Song et al reported improvement in RAND Mental Health Inventory scores between pre-intervention and post-intervention (t (19)=−4.241, p<0.001).55 However, Deave et al reported no significant difference in Warwick-Edinburgh Mental Well-Being Scale score between app and non-app users (median score=54.5 vs 55, p=0.284).64
Coping
Coping outcomes were assessed in two studies; one study reported mixed findings, while one study reported no significant effect (GRADE certainty of evidence: very low).41 59 Gallegos et al assessed the role of mHealth in coping among breastfeeding Australian mothers. The automated text message asked the mothers about their breastfeeding experience, and if their responses expressed some level of distress, a breastfeeding counsellor contacted the woman. As a result, mothers expressed higher levels of active coping (p=0.01) and lower levels of emotion-focused coping (p=0.001) on the Ways of Coping Checklist.41 However, no significant change in the Coping Self-Efficacy Scale scores was reported between pre-intervention and post-intervention in the study conducted by Jallo et al (median score=148.5 vs 155, p=0.129).59
Self-efficacy
Self-efficacy outcomes were assessed in 16 studies.37 41 42 46 48 49 51 53 54 57 58 64 66 69 71 78 Seven studies found positive effects, two studies had mixed findings and seven studies found no significant effect (GRADE certainty of evidence: low). Positive findings were often mentioned during qualitative interviews. Adolescent mothers in the US described a sense of fulfilment, competence and confidence from interacting with text messages, which validated their motherhood role.66 A formula feeding mother in Australia also described a sense of enhanced confidence by using the app.69
However, some quantitative studies reported no change in self-efficacy. Deave et al did not report any change in the Tool to Measure Parenting Self-Efficacy score between baseline and 3-month follow-up (adjusted OR=1.12, 95% CI=0.59 to 2.13, p=0.730).64 Moreover, breastfeeding mothers reported no changes in the Breastfeeding Self-Efficacy Scale score between baseline and 2-month follow-up (M=4.00 vs 4.15) and no significant differences in change over time between intervention and control group (p=0.25).41
Self-management
Self-management was assessed in five studies44 71 72 74 77 of which all reported positive findings (GRADE certainty of evidence: low). Hantsoo et al reported that the intervention group rated their ability to manage their health significantly better than the control group (F=4.03, df=4 and 49, p=0.007) at 8-week follow-up.44 Blackwell et al conducted a mixed-methods study in the US and reported that the proportion of minority immigrant pregnant women likely to strongly agree that the text messages allowed them to have greater control over their prenatal healthcare increased from pre-intervention to post-intervention (28.6% vs 51%, p=0.02).74 In Norway, women with gestational diabetes mellitus who used an app described an increase in feeling of control to manage their own health: ‘I felt that to record [information] in the app was very important…. In that way the app was very important because it gave me a feeling of control’ (p. 105).71
Acceptance
Three studies assessed positive outcomes of acceptance regarding pregnancy and motherhood (GRADE certainty of evidence: very low).53 65 69 In Turkey, Özkan Şat et al reported in the mean subscale score of Prenatal Self Evaluation Questionnaire (PSEQ) that pregnant women who used apps had a better adaptation level to pregnancy than those who did not use any apps (M=18.99 vs 20.86, p=0.005).65 Litterbach et al reported that the app reassured infant-feeding mothers of their feeding decisions and help accept that they were doing the ‘right thing’ for their baby.69
Social support from partners
Partner social support outcomes were assessed in four studies, all presenting positive findings (GRADE certainty of evidence: very low).49 65 68 75 In Kenya, Harrington et al conducted a qualitative study and found that pregnant women and mothers who received text messages on family planning felt improved communication with their partners, which allowed them to start a conversation about family planning.68 Shorey et al reported that parents showed a significant difference in the Perceived Social Support for Parenting score from their spouses compared with the control group who did not use the app (mean difference=27.08, 95% CI=20.94 to 34.80, p<0.001).49 Pregnant women in Turkey who used apps reported lower mean subscale score for the relationship with their husband on the PSEQ compared with those who did not use apps (M=13.28 vs 15.69, p=0.001).65
Social support from healthcare providers
Three studies examined the roles of mHealth intervention in providing social support from healthcare providers (GRADE certainty of evidence: very low).55 72 76 Sixty per cent of low-income pregnant women reported that the two-way SMS encouraged them to put forward more questions to discuss with their healthcare providers and they felt more prepared to see their healthcare provider.55 Pregnant women with diabetes who received informational, motivation and logistical messages via SMS reported that they felt more connected with their healthcare providers.72
Social support from other sources
Ten studies reported on the roles of mHealth in social support from other sources (eg, family, friends and online community).37 38 41 43 56 67 69 74 78 79 Six studies found a positive effect, while three reported mixed findings and one study reported no significant effect (GRADE certainty of evidence: low). Litterbach et al found that the app gave support to infant-feeding mothers during times of need, such as when they were questioning their milk supply and when it was impossible to seek advice from others (eg, in the middle of the night). Mothers who were formula feeding or mixed feeding indicated that the programme allowed them to receive support without fear of judgement regarding their decision to use formula.69 Moreover, Connor et al reported that the app allowed pregnant women and mothers to receive support from the online community through message boards when they could not rely on friends or family.67
Discussion
Findings suggest that mHealth interventions had a positive effect on improving self-management of health and acceptance of pregnancy and motherhood. However, it had mixed effects in anxiety and depressive symptoms, perceived stress, mental well-being, coping, and self-efficacy among pregnant women and mothers. Moreover, mHealth interventions had largely a positive effect on social support from partners, healthcare providers and other sources. Pregnant women and mothers from a socially disadvantaged background, having pre-existing health conditions and behaviours, or dealing with sensitive perinatal issues benefited especially from the mHealth interventions.
mHealth interventions improved self-management and acceptance of pregnancy and motherhood among pregnant women and mothers. This finding is new as Dol et al20 did not report the roles of mHealth interventions in neither outcome. The intervention populations included: pregnant women who are minority immigrants,74 with low socioeconomic status and having depressive symptoms,44 and postpartum women diagnosed with gestational diabetes mellitus.71 These findings suggest that mHealth interventions has the potential to improve self-management of health among pregnant women and mothers who may have pre-existing health conditions and living in resource-limited settings. mHealth can provide ease of access to health education materials and self-monitoring systems where the users can track their own behaviour or health data while also being supported by healthcare providers. Furthermore, three studies reported on the positive roles of mHealth interventions in improving acceptance of pregnancy and motherhood.53 65 69 In Australia, infant-feeding mothers reported that the mHealth intervention provided reassurance to their feeding decisions.69 Infant-feeding mothers could often face difficulties in deciding feeding practices and feel anxious if they made the right decision, especially if they are first-time mothers. mHealth services can potentially provide both informational and emotional reassurance during such decisions.
The use of mHealth largely improved social support from partners, healthcare providers and other sources. This finding is new because Dol et al20 reported that mHealth interventions showed benefits to perceived social support but did not specifically address the source of the social support. A two-way text messaging system in Kenya that provided family planning education to pregnant/postpartum women and their partners improved communication and support between them.68 When family planning education messages are sent directly to men, it is easier for women to communicate effectively with their partners about contraception and partners may gain a better understanding from such communication, leading to more positive attitudes and increased use of contraception.82 Moreover, although the service is not provided in person, mHealth could provide pregnant women and mothers opportunity to use online forums and join groups where they can share and learn from others’ experiences.
mHealth can act as a support system for vulnerable pregnant women and mothers. In South Africa, women undergoing the home phase of medical abortion who received text messages providing timely information on managing their abortion symptoms were more likely to report improved anxiety symptoms than those who did not.39 The messages guided the women through the medical abortion process using a supportive tone without overtly addressing negative emotions. Mothers in Australia who received tailored SMS messages about infant feeding reported that the messages provided support without judgement about their decision to use formula.69 The mothers were reluctant to discuss formula use with healthcare providers because of the fear of being judged. Young women encountering decisions about abortion and infant feeding are at risk of social judgements and discrimination.83 84 Fear of judgement could prevent women from openly discussing their health concerns and delay help-seeking during the perinatal period.85 Findings suggest that mHealth interventions can provide support to pregnant women and mothers who may feel hesitant to seek support in person due to the fear of being judged. The flexible nature of mHealth interventions enables accommodating users’ specific needs and tailoring the programme to their preferences (eg, cultural, literacy, language preferences). This makes it particularly useful for vulnerable populations who often have specific physical and mental health needs.86 The findings add to the existing literature that mHealth interventions reduce access barriers among populations vulnerable to health disparities.87–89
The current systematic review has several limitations. First, high heterogeneity of outcomes was observed among the included studies due to the broad inclusion criteria and search strategy, making it difficult to conduct a meta-analysis. Studies had a wide range of study designs, sample sizes (n=4 to n=2782) and outcome measures (eg, anxiety was assessed with Generalized Anxiety Disorder-7, BAI, HADS), which made the comparison of results difficult. Moreover, positive effects may have been emphasised in qualitative studies and studies with small sample sizes may have reported larger effect sizes.14 Thus, the findings should be interpreted cautiously. Second, environmental factors, such as neighbourhood environment, were not included in our review scope, which could have been important factors affecting the psychosocial health of the given population.90 Third, the current review exclusively searched for articles in English and this may have limited the number of articles identified during our search. Fourth, non-binary terms were not included as search terms and this may have excluded non-binary people from our study. Lastly, the interaction between individual domains of psychosocial health outcomes was not assessed in the current review as it was beyond the scope of the study. Some findings may be a result of the interaction of the outcomes and not necessarily the effect of the mHealth intervention. Despite those limitations, this review addresses research gaps concerning mHealth and pregnancy and postpartum care.
Although the advantages of mHealth interventions have been highlighted, some studies discussed their limitations. Pregnant mothers and women who participated in the mHealth interventions may have been actively seeking help44 46 and may have come from a well-resourced environment with higher socioeconomic status.39 49 Despite the advancement of technology, the digital divide and digital literacy barriers might have prevented socially disadvantaged pregnant women and mothers from participating in the intervention. Moreover, technical difficulties were also reported in a few studies. Such difficulties included operating system limitations (eg, Google’s Android or Apple’s iOS),54 app failure, which reduced engagement,69 and answerability of the system, which created frustration for participants.55 Concerns for data security were also expressed.67 These technical difficulties could have negatively affected the use of mHealth services,91 thus affecting health outcomes. Future studies should consider preventing such difficulties for an effective mHealth intervention.
Conclusions
mHealth plays a positive role in improving self-management and acceptance of pregnancy and motherhood. It also has the potential to provide social support from partners, healthcare providers and other sources. mHealth interventions were especially crucial in improving the psychosocial health among vulnerable pregnant women and mothers. However, some studies reported mixed findings on the effectiveness of mHealth on psychosocial health outcomes. The high heterogeneity and uncertainty across the studies regarding the setting, study design and outcome measures make it difficult to draw firm conclusions; thus, these findings should be interpreted with caution. Future studies using mHealth interventions should consider investigating the context under which mHealth could be more effective while considering its technical limitations in improving psychosocial health among pregnant women and mothers. Furthermore, future studies should also consider the psychosocial health of men transitioning into fatherhood and of same-sex and transgender partners.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplemental information.
Ethics statements
Patient consent for publication
Ethics approval
This study does not involve human participants.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors Conceptualisation—JLS, RRC, MK, AS, EY, MB and MJ. Search strategy—JLS and RRC. Screening—JLS and RRC. Extraction and quality assessment—JLS, RRC and MK. Analysis and interpretation of data—JLS, RRC, MK, AS and MJ. Drafting the manuscript—JLS. Revising the manuscript—JLS, RRC, MK, AS and MJ. Guarantor—MJ. All authors critically reviewed and approved the manuscript.
Funding This research was funded by Program of Bilateral Health and Medical Cooperation between Japan and Russian Federation, Ministry of Health, Labor, and Welfare, Japan.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.